Alveolar bone: structure
The bony makeup of the alveolar process (os al-veolare) has a typical bone structure (Fig 3-20):
- An extremely dense outer bone plate that is covered with periosteum
- An inner bony layer lining the tooth sockets that is greatly perforated
- Spongy bone, which lies between the compact layers
Where the compact layers of the outer surface and the tooth sockets merge marks the bony alveolar crest. The outer layer of the
alveolar bone is the typical cortical substance (substantia corti-calis).
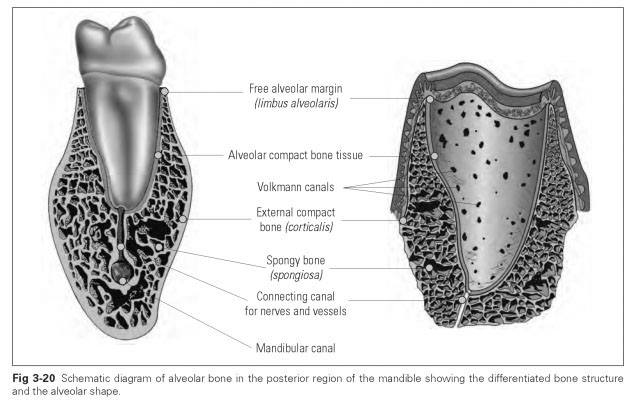
The spongy (cancellous) bone is composed of thin trabeculae, between which the bone marrow is stored. The bone plate of the jaw contains mainly red, blood-forming bone marrow. The spongy trabeculae illustrate the striking functional orientation corresponding to tension and pressure lines initiated by loading from teeth and muscles. The spongy trabeculae can adapt to altered stresses.
The internal alveolar wall to the tooth sockets is a firm, highly perforated cortical layer; it is known as the cribriform lamina (or cribriform plate). It is particularly perforated in the cervical and apical
region. These openings correspond to the Volk-mann canals and link the cementum to the bone marrow cavities through which blood and lymph vessels pass. The embedded bundles of Sharpey fibers can be seen in the cortical layer of the tooth socket in the same way as in the cementum.
The composition of alveolar bone is the same as that of other bones:
- 45% (by weight) inorganic hydroxyapatite of calcium phosphate
- 30% organic matrix of collagen fibers
- 25% water
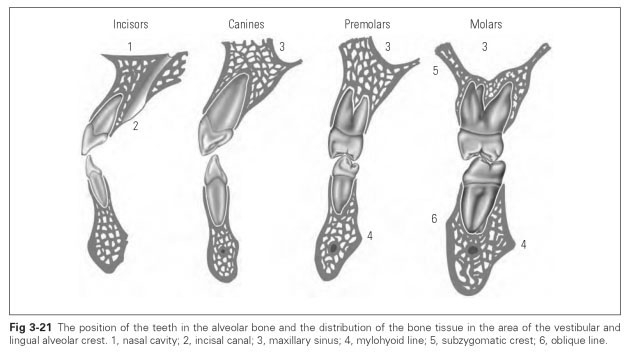
The shape and position of the alveolar bone is determined to a great extent by the teeth and their function (Fig 3-21). For instance, all permanent incisors and maxillary canines, premolars, and molars are inclined in a vestibular direction; the mandibular canine stands rather vertically, while the mandibular posterior teeth show a lingual tendency. The bony layer on the roots is noticeably thin in the external (vestibular) alveolar region of the maxilla, so that the external compact bone and inner cribriform lamina fuse together.
Following tooth loss, the bone lamellae of the sockets are resorbed, and the thin, vestibular bone parts are seen to shrink more than the lingual areas. The alveolar crests appear to be shrinking in a direction of incline, which leads to narrowing of the maxillary ridge and widening of the mandibular ridge crest line.
Bone formation of the maxilla and mandible starts in week seven of fetal life from connective tissue cells. The tooth buds are visible at this stage. When the hard tissue is formed from the bell, thin bone lamellae develop and separate the individual tooth germs.These form the separating walls between the alveoli (alveolar septa), which at birth give rise to ten primitive tooth sockets in each jaw for the primary teeth. The permanent first molars are already noticeable in individual tooth sockets.
The tooth germs are surrounded by the dental follicles, which are later transformed into the periodontal ligament. During root formation and eruption of the teeth, however, the germs also induce growth of the alveolar processes. At the time of birth, the alveolar bones have grown beyond the occlusal level of the tooth germs. Then, during eruption, they grow in line with lengthening of the roots. At the same time, the fiber systems and the cementum for the periodontium develop.
Alveolar processes and alveolar bone develop as jaw components, dependent on tooth eruption, root growth, and differentiation of the periodontal ligament, and are therefore separate from the growth of the other parts of the jaw. During exfoliation and as the permanent dentition emerges, there are similar growth dependencies leading to a complete change of alveolar parts and alveolar arches to make them suited to the permanent dentition.