Centric Relation Splints
Centric relation splints (or simply centric splints) initiate self-centering of the condyles in the fossae, as established via a centric record. With the physiologic (relieved) joint position, neuromuscular relaxation is achieved, a pain-free therapeutic position is created in the case of intra-articular disorders, or pretreatment is undertaken for extensive occlusal correction (eg, in an abraded dentition).
Centric relation denotes the physiologic condylar position, a joint-related occlusal situation in which both condyles lie pressure-free in the centric position in the articular fossae. This position can be contrasted with maximal intercuspation. Therefore, the centric position of the condyles must be registered and transferred to an articulator to fabricate a centric relation splint.
Cranium-related transfer of the maxillary model takes place in an articulator, in which the patient's movement parameters (eg, condylar path inclination, Bennett angle) can be set. For the inter-occlusal record registration, the patient's nerves and muscles must be relaxed; ie, the patient must be capable of achieving the centric position. This neuromuscular relaxation can be produced by prior treatment with reflex splints.
Variable types of centric relation splints are identified, as reflected in the following terms:
- Occlusion rim and relaxation plate
- Equilibration splint
- Michigan splint
- Stabilization splint
- Occlusion-raising splint
Vertical opening is produced with the centric relation splint, where the antagonists are positioned in punctiform, flat, but stable centric stops. The occlusal height lies within the interarch distance, and the horizontal relation is ground in the form of occlusal depressions for the active cusp tips (Fig 11-11). The grinding must be constantly adapted to the changing jaw relations.
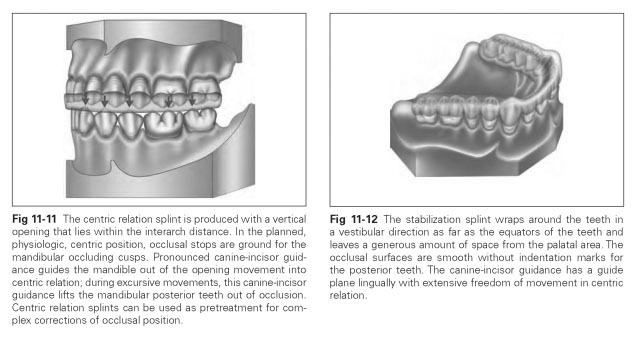
In protrusive and laterotrusive excursions, the posterior teeth must be lifted out of occlusal contact, which is achieved with anterior canine guid-ance.The centric relation splints are fabricated for the maxilla and extended onto the palatal area to ensure sufficient stability. A centric relation splint can also be made into a prosthetic splint with artificial teeth for temporary replacement of support areas. In total tooth loss, centric relation splints are used to try out increases in occlusal height or removal of functional disorders.
The splint can be carved in wax and converted into acrylic or produced with self-curing or light-curing acrylics. After insertion of a centric relation splint, the centric contacts are ground until the contacts remain stable on the splint; aftercare is needed to grind off interfering contacts.The splint is worn all night and during the day as often as possible. Once the symptoms have subsided, the splint can be withdrawn after a few weeks' wear.
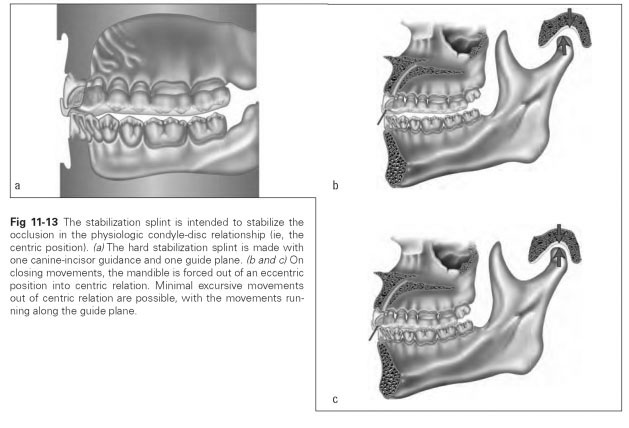
A stabilization splint is regarded as the standard appliance among centric relation splints and is used for painful, tense muscles; in cases of TMJ arthritis for relieving the joint structures; as a pre-prosthetic therapeutic aid; as well as in cases of advanced periodontitis. It is mainly worn at night, and wear is gradually reduced as the symptoms diminish.
The splint is fabricated from hard acrylic for the maxilla, covering all the teeth and keeping the occlusal surfaces flat. The acrylic wraps around the teeth to just above their equators (Fig 11-12). Guide planes for the anterior and posterior teeth can be incorporated to enforce canine guidance or canine-incisor guidance for the protrusive and lateral movements of the mandible (Fig 11-13).
Fabrication of the splint is performed on precisely mounted models (wax centric relation record, facebow) so that grinding can be done in the articulator. The splint can be carved in wax, invested, and fabricated by a hot-pressing process. On the maxillary model, the profile of the splint border is marked approximately 1 to 2 mm cervically below the tooth equators; a minimum distance of 1 mm to the marginal periodontium must be maintained. In the anterior region, the splint border projects only 1 mm beyond the incisal edge; the palate is avoided in a U shape. An occlusal elevation of approximately 2 to 3 mm is performed to ensure the minimum material thickness occlusally.