Characteristic Features of Tooth Forms
The previous descriptions of dental substances and the tooth attachment apparatus (periodontium) referred to the law of form and function. The connection between form and function also applies when describing the different tooth forms. It explains the extent to which the teeth and the tissue involved form a unit, having developed and grown for their particular functions and hence taken on a particular form. Every characteristic feature of the form of dental tissue therefore indicates a particular significance.
Any replacement tooth will have an influence on the function of the whole masticatory system. Tooth forms should be seen not only as esthetic features but above all as functional forms developed for specific tasks. Dental technicians must be familiar with the tooth forms down to the smallest detail because they are constantly faced with the task of skillfully producing individual teeth for individual dentitions. The dental technician hence needs to recognize anatomical details not only as characteristic features of form but also as functional necessities. The individual teeth are therefore described herein with considerable accuracy, although there are some characteristics of form that are common to all teeth.
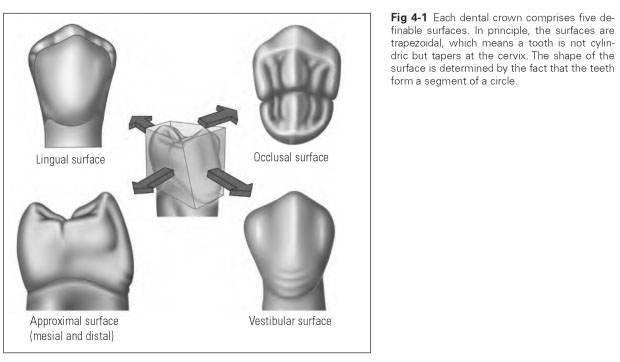
Every crown of a tooth has five definable surfaces, which are named after the directions in which they face (Fig 4-1):
- Occlusal or masticatory surface (facies occlusalis; facies = surface)
- Vestibular, buccal, or labial surface (facies vestibularis)
- Lingual surface (facies lingualis)
- Mesial approximal surface (facies approximalis)
- Distal approximal surface
The occlusal surface indicates the terminal occlusion or occlusal line in which the teeth rest when biting together. On the posterior teeth this is a true surface, bearing cusps, that fits into the surface of the antagonist (opposing) tooth and is suitable for crushing food (Figs 4-2 and 4-3). It is defined as a true chewing surface and therefore is also known as a masticatory surface (masticare = to chew). On the anterior teeth, this surface is reduced to a thin edge and is known as the incisal margin or cutting edge. The incisal margin of the anterior teeth is suitable for shearing food (Fig 4-4).
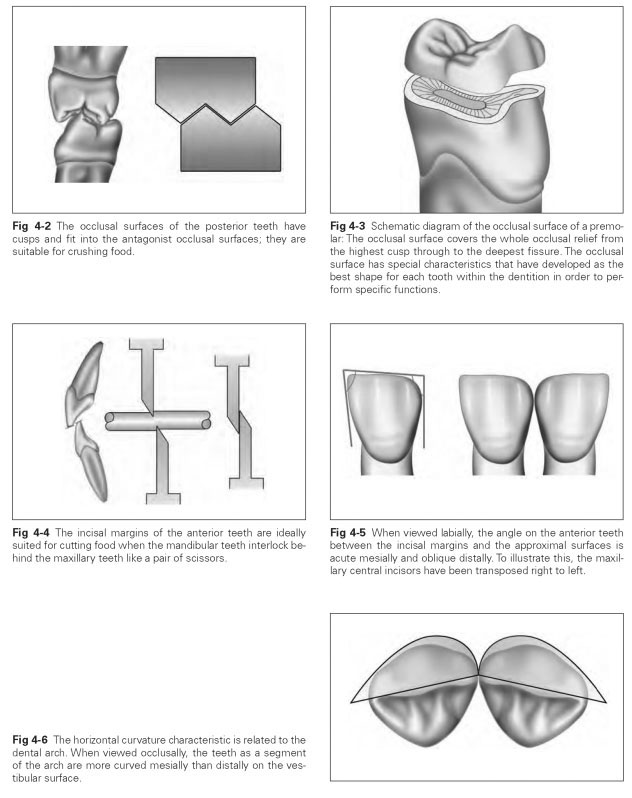
The angle characteristic denotes the angular transition from the occlusal contour to the ap-proximal surfaces. Looking at the teeth from the vestibular aspect, it can be seen that the occlusal surfaces or incisal margins recede distally; the teeth are higher mesially than distally. Looking at the whole dentition from the vestibular aspect, it is also noticeable that the relative height of the teeth decreases in the distal direction. On an incisor, the transition from the incisal margin to the approximal surfaces mesially is sharp-edged, while the distal transition is rounded and oblique.
Because the pronounced acute angle is always mesial, it is possible to tell from the angles which side of the mouth an anterior tooth belongs to (Fig 4-5).
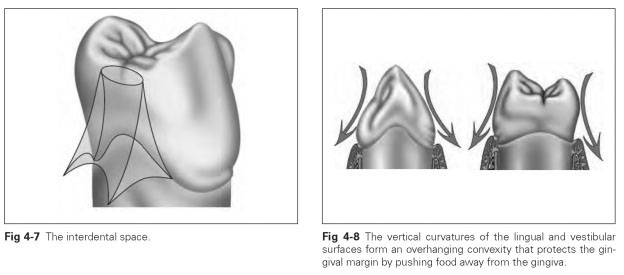
The vestibular surface is the surface that faces the vestibule, ie, is oriented in a buccal or labial direction or facing the outer surface. This surface gets narrower toward the cervical region and wider toward the occlusal surface. Viewed approxi-mally, the vestibular contour bulges outward in a curve at the cervix and is concave occlusally. At the neck of the tooth, this produces an overhanging "belly" that protects the gingival margin. Food is pushed over this bulge away from the margin of the gingiva.Therefore, this bulging form of the vestibular surfaces must be re-created in prosthetic crowns. This curvature is also described as the vertical curvature characteristic and is most pronounced in the mandibular teeth.
The horizontal curvature characteristic or characteristic of mass denotes the marked transverse convexity of the vestibular surface. The surface contour, when viewed occlusally, is more curved or bulging in the mesial part, while it recedes flatly on the distal side (Fig 4-6). The position of the tooth in the dental arch can be classified by this mesiovestibular distribution of mass, which is why it is also referred to as an arch characteristic. If it is known whether a tooth is maxillary or mandibular, the side of the mouth to which it belongs can be identified by the curvature characteristic. The curvature and angle characteristics must be reproduced on a prosthetic tooth so that it fits precisely into the existing dentition.
The lingual surfaces of the teeth face the tongue; in the maxilla, this surface may also be known as the palatal surface (facies palatina). The lingual surfaces are always smaller than the vestibular, which is due to the arrangement of the teeth in the dental arch. When equal slices are cut out of a circular area, the outer surface is bound to be larger than the inner surface.
The lingual surface is also convex, but the widest curvature lies in the middle and is not reduced toward the cervix. The lingual surface always tapers toward the occlusal area, where it becomes the occlusal or masticatory surface.
The approximal surfaces are the mesial and distal areas of contact with the neighboring teeth; this is where the points of contact with the adjacent teeth lie, which is why these are also known as contact surfaces (facies contactus). Approximal surfaces are basically trapezoidal: The long baseline is at the cervix, while the short line is toward the occlusal surface, and the contour lines of the lingual and vestibular surfaces form the sloping lines. Viewed lingually or vestibularly, the bulging convexity of the approximal surfaces can be seen to lie directly occlusally or incisally and not at the neck of the tooth. The tooth is thus wider occlusally.
On a tooth, a distinction is made between a mesial and a distal approximal surface.The distal approximal surface is usually smaller than the mesial, but they only differ slightly in their basic form.
Contact points result from the convexity of the approximal surfaces of two adjacent teeth and lie just below the occlusal line. The teeth touch each other above the contact points. As a result, they can support each other (ie, provide reciprocal anchorage) if they are moved sideways or tipped lingually. Then they do not have to bear the sideways pressure alone but can spread the strain to the whole dentition.This is why the contact points are so important and must be re-created in prosthetic crowns. When a tooth is missing, this support mechanism within the dentition is disrupted. Then sideways pressure can very easily lead to excessive strain and damage to the periodontium.This is why even a single tooth within a dentition should be replaced.
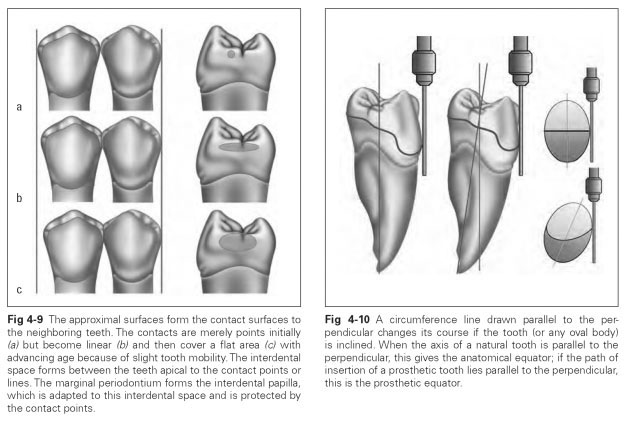
Interdental space denotes the space between the teeth that is apical to the contact points and filled with gingival tissue; this is where the interdental papilla lies (inter = between) (Fig 4-7). If the teeth are very tightly packed together at the contact points, no food particles can be squeezed between the teeth; the contact points protect the gingival papillae (Fig 4-8).The approximal contact point, which is initially merely a point in young people, becomes linear over time and then is worn away to create a flat area owing to slight tooth mobility with advancing age (Fig 4-9). This makes the teeth crowd closer together in a mesial direction and is referred to as physiologic mesial migration. If a tooth is missing, the adjacent teeth lean into the gap.
All the surfaces of a tooth put together show that a tooth is not cylindric in shape but concave at the neck, only getting wider coronally and becoming concave again toward the occlusal surface. Therefore, the dental crown is always undercut. This bulging shape serves the purpose of deflecting food or forming the approximal contact.
The anatomical equator is the curvature line of the widest circumference of the dental crown.The course of the convexity around the tooth can be traced. Using a black lead pencil to draw a line around the tooth parallel to the vertical dental crown axis, the anatomical equator or the curvature line can be marked. The course of this equator is not at a single height; approximally it runs close to the occlusal surface and vestibularly or lingually close to the cervical region.
The prosthetic equator denotes the widest circumference line on the prosthetic dental crown, with reference to a freely chosen perpendicular at which the tooth is tipped. If a path of insertion for the denture is fixed during fabrication of partial prostheses, the teeth will be at a different incline to that.The prosthetic equator is obtained by running a black lead pencil parallel to the insertion path around the tooth.
To summarize, the reference line for the anatomical equator is the natural tooth axis; for the prosthetic equator, the reference line is a freely chosen path of insertion that does not necessarily coincide with the tooth axis (Fig 4-10).