Developmental Anomalies of the Jaws
The development of the jaw starts around the end of the third week of embryonic life. The normal development process can be interrupted by malformations due to inhibitory factors, by which palatine tori do not develop fully and fail to fuse together in the midline.
Normal fusion advances like a zip fastener, closing from front to back as far as the uvula. If union of the palatine processes at the median palatine suture does not take place, this gives rise to a cleft palate extending from the incisive foramen to the uvula, which is also split. There are numerous degrees of severity, from a complete cleft through to a uvular cleft (Fig 9-2); clefts that only affect the soft palate may be referred to as velar clefts.
Forms of cleft lip, jaw, and palate
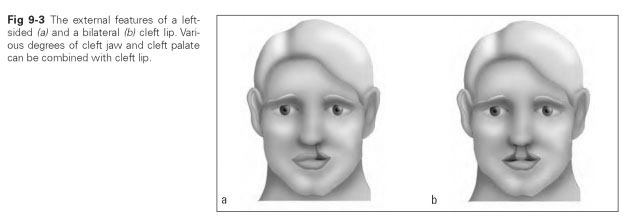
Cleft lip (cheiloschisis) denotes a split in the upper lip. This form can be surgically closed during the fourth to sixth month of life with a good functional and cosmetic outcome. Left-sided cleft lip is twice as common as right-sided, or the cleft may be bilateral (Fig 9-3); a cleft in the middle of the lip is very rarely seen.
Partial clefts of the lip, at their least pronounced, are evident as slight furrows in the red of the lips or as a small dent next to the philtrum. Cleft lip can be found in every possible combination with cleft palate.
Cleft jaw (gnathoschisis) denotes a split of the maxilla because the incisive bone has not grown together with the maxilla at the intermaxillary suture. It usually occurs in conjunction with other cleft deformities.
Isolated cleft palate (palatoschisis or uranoschi-sis) is a malformation of the hard and soft palate where the whole palatine vault is split along the median palatine suture.
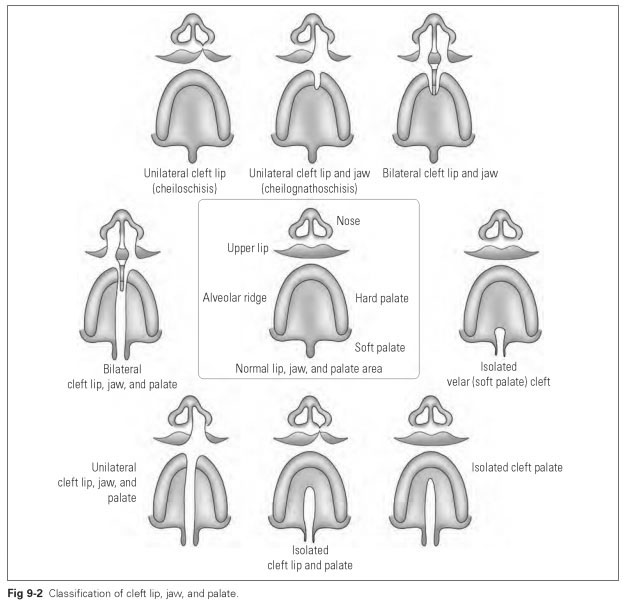
Complete cleft (cheilognathopalatoschisis or cheilognathouranoschisis) is a cleft palate combined with bilateral cleft lip and jaw. This most severe form of cleft is twice as common in males as in females. The abnormality in development of the palate, jaw, and lips is usually accompanied by anomalies of the tooth germs in the region of the cleft. For instance, delayed growth or schizodontia (development of twin tooth forms) of the incisors may occur in both the primary and the permanent dentition. Frequently, individual teeth may be entirely absent, or several teeth may erupt.
In fact, anomalies of tooth formation often occur outside the cleft area as well. There is evidence that cleft formation and development of the wrong number of teeth (too few or too many) have causes in common.
The developmental anomaly in the form of cleft lip, jaw, and palate leads to stunting of the maxilla, while the mandible grows to normal size.This creates an impression of prognathism and hence protrusion of the mandible.These complete clefts result from the combined effect of congenital and environmental factors or damage caused by medication; they are therefore a multifactorial condition.
Developmental anomalies in the primary dentition
If there is no abnormality in the shape of a complete cleft, the primary dentition will develop normally. Malposition of teeth is relatively rare and only slightly pronounced.
Typical anomalies in the immediate area of the mouth include the following:
- Tongue doubling, shortening (microglossia), absence (aglossia), or cleft
- Medial cleft of the mandible
- Duplication of the maxilla and the mandible (not viable)
- Underdevelopment of the mandible (hypoplasia)
- Crowding if a few primary teeth are duplicated
- Premature eruption of the primary teeth and permanent teeth; premature dentition (primary dentition complete after first year of life, permanent dentition complete after third year of life)
Facial clefts refer to various forms of malformation due to inhibited development, such as nasal, eyelid, forehead, lower lip, or tongue clefts, which are mostly associated with anomalies of tooth position and displacement of occlusal position. The oblique facial cleft (meloschisis) extends from the upper lip to the eye, while a transverse facial cleft (macrostomia) widens the oral orifice at the sides. Facial clefts can be remedied in several operations, the aim of which is to achieve normal anatomical forms with sufficiently esthetic conditions and to establish masticatory function and phonetics. In most cases, orthodontic treatments are required as well as the surgical procedures.