Transferring Forces for Tooth Movements
Forces are transferred to teeth by means of orthodontic appliances, and these forces are evident as tensile and compressive effects in the periodontium and produce the necessary remodeling stimuli. Every tooth movement causes areas of compression and tension in the
periodontal ligament, the extent of which depends on the type of movement. Tipping movements produce neutral areas around the center of rotation in the middle of the root, while the pressure and tension peaks are found at the root apex and the alveolar margin. During a parallel shift of a tooth, the areas of compression and tension arise throughout the length of the root.
The transfer of forces to the teeth should initiate directed movement, which is why it is necessary to know precisely the effect of a force being exerted (Fig 10-10). Except in intrusion (sinking) or extrusion (lifting out) of a tooth, the forces for tooth movement will always act perpendicularly to the tooth axis. A force emanating from an orthodontic appliance to achieve rotation of a tooth will have to act differently on the tooth than a force intended to achieve parallel shift or tipping of teeth. A distinction is made between single-point, two-point, and multipoint application of force.
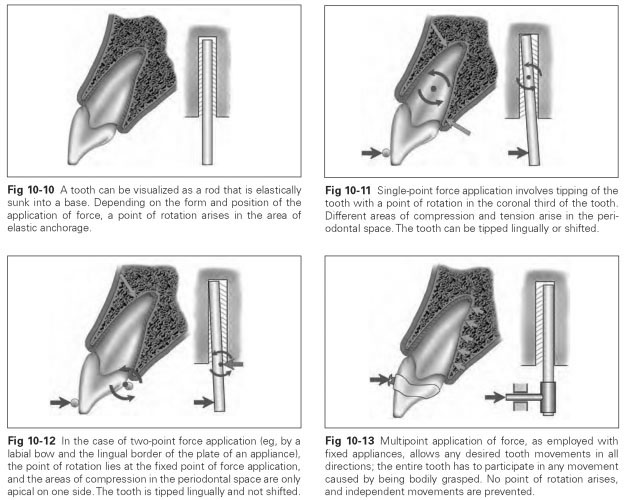
Single-point force application means the transfer of forces to teeth for guided orthodontic movements in which a force acts at a right angle to the tooth axis and produces tipping of the tooth (Fig 10-11). The connection between tooth and jawbone provided by the periodontal ligament does not act like a joint with a fixed point of rotation, but the position of the point of rotation can be variably influenced, depending on where the point of force application is located.
A single-rooted tooth with a conical root acts as a two-arm lever where the tipping axis lies roughly in the apical third of the tooth. However, the tipping axis is not fixed, and its position can change within the bottom half of the root as a result of the length of the coronal lever arm protruding out of the jaw and the position of the point of force application. Irrespective of the definitive position of the tipping axis in the apical half of the root, areas of compression arise in the periodontal space, around the apex of the root, and in the marginal area, with opposing areas of tension. The loaded areas increase in intensity with the distance from the point of rotation; the neutral area is located at the point of rotation itself. The loading strength is directly dependent on the magnitude of force applied and the position of the point of force application in relation to the point of rotation. The greater the force applied and the longer the lever arm (the more coronally the force is applied), the greater will be the compressive and tensile loading in the periodontal tissue.
Two-point force application or semirigid force application is a force couple with which eccentric tipping and rotations can be produced (Fig 10-12); a rotated tooth can also be regulated by such a couple. The tooth movement can be influenced by the precisely defined position of the tipping axis. All that is required is to fix—by means of an abutment—the point of rotation for the tooth movement relative to the application of force. If a clasp engages labially in the incisal third of the crown, a rigid abutment can serve as the point of rotation in the palatocervical position. In other words, a spring clasp presses from labially against the tooth, which is grasped on the rear by the appliance plate. Now the tooth is tipped over the border of the plate.
As a result, the position and intensity of the areas of tension and compression in the periodontium are altered. In fact, only one area of compression and tension arises in the apical region of the root.
Multipoint force application precludes any independent movement of a tooth. If the tooth is grasped bodily and the "grasping" device is moved, the whole tooth must adapt to this movement (Fig 10-13). This principle is put into practice with fixed appliances when the tooth being moved is bodily grasped by a broad metal band and this band is moved without distortion by a square arch. The tooth has to participate in any type of tipping, rotation, and parallel shift of that band. The attraction of multiband appliances actually lies in the possibility of successfully carrying out any chosen tooth movement by means of this principle of multipoint application of force.
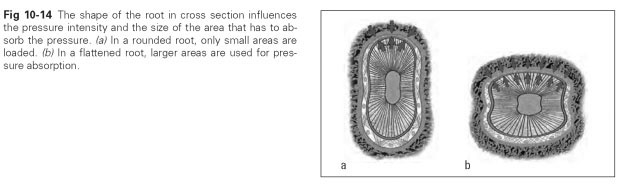
The forces for tooth movement at first appear to originate from the appliance. They are absorbed by the teeth (Fig 10-14), passed on to the periodontal tissue, and from there transferred so that the remodeling stimuli can act on the bodies of the jaws, the sutures, and the TMJs. The appliance itself must be suitably supported to produce the necessary forces.